
Research Article | DOI: https://doi.org/10.31579/2578-8965/007
*Corresponding Author: Jennifer Rovira Pampalona, Department of Obstetrics and Gynecology, Consorci Sanitari de l’Anoia. 11 Catalunya Avenue, Igualada, 08700. Barcelona. Spain, E-mail: Jenny_rovira@yahoo.com
Citation: Jennifer Rovira Pampalona, Daniel Vega Moreno, Maria Degollada Bastos, Àngel Guerra Garcia, Joan Carles Mateu Pruñonosa , Pere Bresco Torras, Influence of Emotional Status on the Pain during the Outpatient Hysteroscopy. J.Obstetrics Gynecology and Reproductive Sciences, 2(1); doi. 10.31579/2578-8965/007
Copyright: © 2018 Jennifer Rovira Pampalona et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 February 2018 | Accepted: 17 March 2018 | Published: 11 April 2018
Keywords: Outpatient hysteroscopy, polipectomy, pain, visual analogical scale, anxiety, Hospital Anxiety and Depression Scale (HADS)
Introduction:
The outpatient hysteroscopy is a minimally invasive technique, well tolerated by the majority of patients. However, the pain appears in a considerable percentage of patients, and this is the leading cause of failure. There are different factors related to pain. The aim of the present study is analyzing the association between emotional status and pain perception during the outpatient hysteroscopy.
Material and methods:
A retrospective survey. It was composed of 192 patients with sonographic diagnosis of endometrial polyp. An outpatient hysteroscopy was conducted from March 2013 to January 2015.
Socio-demographic data and obstetrician history were collected. The intensity of pain during the test was evaluated by means of EVA, as well as the emotional state by means of Hospital Anxiety and Depression Scale (HADS).
Results:
The average score in VAS was 5.06. Regarding the score in HAD, it was 6.87 in anxiety and 4.25 in depression. For the entire sample, a positive correlation was evidenced between the intensity of pain (VAS) and the level of depressive symptomatology (HAD depression; p=0.001). This correlation was not shown in patients with anxiety symptomatology (p>0.05). The patients who did not succeed during the procedure, a correlation with the pain perception was observed, with a higher punctuation in VAS and depression scale (p<0.05).
Conclusion:
There are some factors such as the emotional status of the patient which could modulate the perception of the pain, showing a positive correlation between them. This is an important issue to considerer for the success of the ambulatory hysteroscopy.
Hysteroscopy has become a fundamental technique in the usual gynecologic practice due, in part, to some technological advances in the field of endoscopy as well as its high availability and low rate of complications.
The outpatient hysteroscopy involves the study for the complete evaluation of the uterine cavity [1], and it means an important change regarding the techniques used previously [2]. Nowadays, and due to the advances that have taken place during these last years, the surgical part has been integrated in the diagnostic procedure, and therefore the outpatient hysteroscopy with the subsequent surgical bypass has become both a diagnostic and therapeutic procedure [3].
All of all, the outpatient hysteroscopy could be understood as minimally invasive technique well tolerated by the patients [4]. However, in a considerable percentage of patients the pain appears as the leading cause of procedure failures [5]. A number of factors related to pain have been identified in previous studies, such as cervical stenosis, previous surgeries, nulliparity, or menopause, among other causes that are considered inconclusive evidence until now [6]. On the other hand, it is important to highlight that nowadays the use of paracervical anesthesia and/or oral analgesia for the pain during the hysteroscopy procedure is a controverted issue [7,8].
The emotional status has been associated with the pain perception during most of the surgical procedures and, particularly, with the outpatient hysteroscopy [9]. For instance, a high level of anxiety might predict the pain during the procedure and 60 minutes after.
Despite conventional medical and surgical procedures have focused on the first dimension of pain, it is well known that the emotional status of the patient can modulate the pain threshold. In line with this, for example, previous studies have shown that depression is more prevalent in people with pain [10], In addition, previous findings showing an analgesic effect (REF) of some antidepressants [11] (REF) and studies suggesting a role of the same brain regions on both the negative affect and pain (REF), also supports this claim.
Nevertheless, it is important to note that nowadays there are only few studies analyzing the role of the emotional status on pain perception during the outpatient hysteroscopy [12]. The aim of the present study was to analyze this association. First, we described the anxiety and depression levels in patients who carried out an outpatient hysteroscopy. Second, we analyzed the relationship between the pain intensity and the psychological distress (anxiety and depression). Finally, we explored the possible differences between the pain intensity and the psychological distress among those patients whom the hysteroscopy was not successful. In accordance with previous studies, we hypothesized a relationship between the level of pain and anxiety and the depressive symptomatology in the sample of our study. We also expected higher levels of pain, anxiety and depression in those patients who suffered an unsuccessful hysteroscopy (in comparison with patients who experienced a satisfactory outcome).
A retrospective study was carried out. We reviewed a database conducted by our group in a previous clinical trial (JEN-HTS-2013-19). A total of 192 patients with sonographic diagnosis of endometrial polyp (> 1 cm) were included in the study. Participants underwent an outpatient hysteroscopy (performed in Igualada’s Hospital, Barcelona, from March 2103 to January 2015). Socio-demographical information was gathered and it can be show in the Table 1.
All patients were randomized as it is described in Rovira et al. The hysteroscopic system used, which were randomized for each patient, were the TRUCLEARTM 5.0 Tissue Removal System (Smith&Nephew) with mechanical energy in 52.6% of patients and the Versapoint® Bipolar Electrosurgery System (Gynecare; Ethicon Inc.) with bipolar energy in the other 47.4% patients.
The TRUCLEAR 5.0 System consists of a 5 mm Hysteroscope with a 0º direction of view and a 5.6 mm sheath. The tissue removal device has a distal window that captures intracavity pathology and resects it to the base through a rotating cutting edge and simultaneous aspiration.
All procedures involving the Versapoint® Bipolar Electrosurgery System were carried out using the 3 mm Olympus® Rigid Hysteroscope, which has a 30⁰ direction of view and a 5.5 mm sheath. The Electrosurgery instrument used was the Versapoint® Bipolar Twizzle Tip Electrode (Gynecare; Ethicon Inc., NJ, USA) which is inserted through the working channel (5Fr) of the hysteroscope.
Once included in the study, patients were randomized to 4 groups: group 1 was staff experienced in using the TRUCLEARTM System, group 2 was staff experienced in using the Versapoint® System, group 3 was staff undergoing training in using the TRUCLEAR System and group 4 was staff undergoing training in using the Versapoint® System. Patients randomized to groups 1 and 2 were treated by the same senior surgeon (MDB), who has over 10 years of experience with the Versapoint System and over 2 years of experience with the TRUCLEARTM System. Patients randomized to groups 3 and 4 were treated by three junior surgeons, who were 4th -year obstetrics and gynecology residents and receiving training in hysteroscopic techniques (ERG, JRP, PV.)
The procedures were carried out in ambulatory care with no anesthesia or sedation of any sort. No cervical or endometrial preparation was performed pre-intervention.
All participants completed a self-report assessment when the procedure was finished. First, a Visual Analogue scale (VAS) was used to assess the intensity of pain during the procedure. It is a measure that captures the subjective perception of pain experience. Respondents specify their level of agreement to a statement by indicating a position along a continuous line between two end-points no pain, maximum pain. Previous studies have shown that the VAS is a useful scale when measuring pain intensity. Second, the emotional status was evaluated by means of the Hospital Anxiety and Depression Scale [14] (HAD). This scale is a self-reported test that asses anxiety and depression in inpatient settings (not psychiatry). This scale is a good instrument to detect the negative effect (psychological distress) in non-psychiatric patients since it does not include somatic symptoms of anxiety and depression. The HAD is composed of 14 items, with subscales of anxiety and depression. The option range is from 0 to 3. The range from 0 to 7 indicates no anxiety/depression; from 8 to 10 will be taken into consideration, and from 11 to 21 indicate relevant symptomatology and a probable case of anxiety and depression.
All the patients were instructed in the correct use of each scale.
Other variables were assessed: Data socio-demographic and obstetrician antecedents (parity: nulliparous, 1 delivery, more than one delivery; type of delivery: vaginal vs. cesarean; hormonal status: menopause vs. no menopause).
For the statistical analysis, we divided the sample according to the result of the hysteroscopy. Thus, we considered a successful outcome when we achieved the correct entry into the uterus cavity, the entire view with exeresis and the complete extraction of the intracavitary pathology.
Statistical analysis was performed using SPSS v17. First, descriptive data analyses were carried out. Second, since two different hysteroscopic techniques (Versapoint vs. Truclear System) were used, an ANOVA analysis was performed to rule out possible differences. In this analysis, we included Hysteroscopic (Versapoint, Truclear System) as between-subject factor and Anxiety (HAD anxiety scores), Depression (HAD depression scores) and Pain (VAS scores) as within-subject factor. Third, bivariate correlational analysis was also conducted to analyze the relationship between HAD and VAS scores. Finally, a possible difference between groups on hysteroscopy outcomes (success, not success) was tested using a Pearson´s Chi-square test (χ2) for the categorical variables and two-tailed independent Student’s t-test for VAS and HAD.
The clinical trial (Rovira et al.) was approved by the Bellvitge University Hospital Clinical Investigation Ethics Committee (Reference #AC147/12), with Sponsor Protocol Code JEN-HTS-2013-19.
The average age of all the patients included in the study was 53.63 ages (+ 13.88). We describe the most important characteristics in table 1.

Table 1. Socio-demographic characteristics and obstetrician clinical.
There were no statistically significant differences in pain reported by patients in either
group. Patients who underwent Versapoint and Truclear System showed similar scores in pain intensity (Versapoint, mean score = 5.24, S.D.= 2.65; Truclear System, mean score = 4.80, S.D.= 2.49; P = 0.24), anxiety scores (Versapoint, mean score = 6.88, S.D.= 3.71; Truclear System = mean score = 6.86, S.D. = 4.36; P = 0.97) and depression scores (Versapoint, mean scores = 4.35, S.D.= 3.96; Truclear System, mean score = 4.14, S.D.= 4.05; P = 0.71). These results suggest that that pain intensity and psychological distress were independent of the hysteroscopy technique.
For the totality of the patients, we found an association between the pain intensity (VAS) and the depressive symptomatology (HAD depression; r= 0.237, P = 0.001). In contrast, no association was evidence between the pain intensity (VAS) and the anxiety symptomatology (HAD anxiety; r= 0.114, P> 0.05).
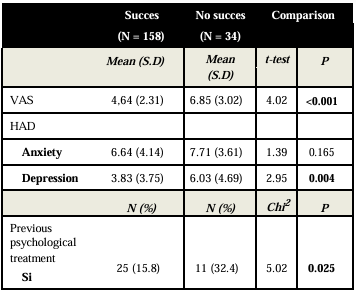
Table 2. Descriptive information between success versus no success during hysteroscopic procedure.
The success rate of the hysteroscopy was 79% (n=158). In table 2, we can observe the difference between patients with a success during hysteroscopy versus the group without success during de hysteroscopic procedure. It is important to highlight that patients with unsuccessful outcome in the surgery, exhibited higher levels of pain (VAS) and depression (HAD) before such intervention.
Despite the growing interest in the outpatient hysteroscopy as a secure and well tolerated procedure, nowadays the reasons by which pain is present in some patients remains little understood. In the current study, we address this important question assessing a large sample of patients. Results suggest a positive relationship between the severity of prior depressive symptoms and pain intensity during the outpatient hysteroscopy. In addition, an important finding of the current study was that patients who experienced a negative outcome in the hysteroscopy (versus positive outcome) showed high depressive symptomatology prior to surgery and increased pain intensity during the procedure.
To understand the pain and the emotional status relationship, it is important to highlight the multidimensionality of a painful experience, where sensoperception mechanisms play a partial role in the processing of this complex phenomenon. In this vein, Melzack and Casey (1968) described pain in terms of three dimensions: (i) sensory-discriminative (e.g., sense of the intensity, location), (ii) motivational-affective (e.g., unpleasantness and urge to escape from it), (iii) cognitive-evaluative (e.g., pain appraisal, cultural load). While the sensory-discriminative dimension is directly associated with the anatomic and physiologic mechanisms and the nociception, the rest are related to the emotional status of the patient.
The assumption of the minimal invasiveness of outpatient hysteroscopy is supported in their benefits when comparing it with other techniques as dilatation and curettage or hysteroscopy in an operation room. In this vein, outpatient hysteroscopy involves substantial benefits for the patient including less complications and faster recovery [15,16] the reduced anxiety associated with undergoing the procedure immediately, a dislike of general anesthetics and the convenience of not disrupting usual routines, and the public health system, in terms of efficient resource utilization by translating inpatient workload in an outpatient setting. For this reason, for the last few years, different innovations have been introduced in the field of outpatient hysteroscopy in order to minimize patient discomfort and promote the chance of success of the procedure [17].
However, the idea that a medical procedure is minimally invasive does not always consider the emotional experience of patients (see: Gambadauro, Navaratnarajah and Carli 2015 (14). The psychosocial aspects of care were also identified as important in assisting women to cope, and form a key factor influencing patient’s evaluation of procedure. The outpatient hysteroscopy is a relatively short procedure and it is preferred by most patients. This type of procedure is normally performed without any cervical preparation or anesthetic. Thus, the expectation that increasingly invasive diagnostic and therapeutic procedures will be performed in the outpatient setting for the patient might be perceived as a stressful situation. And this is associated with an increased anxiety and the emotional state with psychological and physiologic responses.
In fact, only few studies include an assessment of emotional distress in their surgery protocols. Our results are partially in line with previous studies.
The finding of an association between depression and pain in the sample of study suggest a co-occurrence of these two phenomena in patients undergoing an outpatient hysteroscopy. This type of information is extremely relevant in the context of modern patient setting care.
On the other hand, contrary to our hypothesis, no association was found regarding pain levels and anxiety symptoms. Previous studies remark the anxiety as an important problem in surgeries that has also negative repercussions and consequences before and after the procedure [18]. It is important to know that pain is not an emotionally neutral experience but is almost always accompanied by emotional disturbance and distress. In some patients, the anxiety might become like painful experience and increased the likelihood of intolerance for the outpatient procedure. We should consider the pain the most important point related on failed rates in the outpatient hysteroscopy. It has some repercussion in the efficacy and efficiency of the technique.
The main objective of the study of Kokanali MK et al. (15) was establishing whether there was any correlation between the anxiety levels before the procedure with referred pain for the patient during and after (60 minutes) the outpatient hysteroscopy procedure. Some questionnaires [State-Trait Anxiety Inventory-Trait (STAI-T) and State-Trait Anxiety Inventory-State (STAI-S)] which evaluated the usual anxiety status and the anxiety during the procedure were used. And the VAS was also used to evaluate the pain. The scores obtained were directly related to the pain score showed by the patient during the procedure. After 60 minutes, only the patients with high scores in STAI-S scales (state of permanent anxiety) showed a positive and significant correlation with the pain.
Other factors, not directly linked to the patients, may be the cause of anxiety before the hysteroscopy. Carta et al. [19] found that having to wait 60 minutes or more for the procedure is associated to a higher likelihood of pain.
It is already known that the pain perception is a subjective and multifactorial experience. This could be modulated by the emotional state of the patient, because of both their anxiety level and emotional status [20]. For this reason, the pain perception in two equal stimuli could be different in each one [21].
There are other psychosocial aspects which have been studied as modulated factors helping the patients to cope with the pain experienced during the procedure like the woman’s relationship with the doctor and nurse undertaking the procedure, or the possibility to watch the television screen during the hysteroscopy procedure [23].
Importantly, in the present study we analyzed differences between those successful versus failed hysteroscopies, focusing on pain perception and emotional status (anxiety and depression). We found that patients in failed intervention showed higher levels of pain and depression in comparison with patients in successful hysteroscopy. This important finding suggests that the patients with higher scores in the depression scale (HAD) has less tolerance during the procedure. It involves that sometimes the hysteroscopy must be finalized and the patient has to be referred to surgical room in order to carry out the same procedure with anesthetic.
In our hospital, according to established protocols, no patients had cervical preparation or any type of anesthesia. It is well known that in order to improve the patient tolerance during the hysteroscopy entry through the endocervical channel, mainly in nulliparous and menopause patients, some medication such as mifepristone and misoprostol has been recommended by some authors before the hysteroscopy procedure [23,24]. The menopause status induces atrophy that often causes formation of tight stenosis or persistent synechiae that makes the introduction of the hysteroscopy [25] difficult. However, some authors proposed the use of analgesia or anesthesia before the procedure. But the studies that have been published up to now have failed to demonstrate any significant benefits in some of these cases. Therefore, there is no consensus on its correct use [26-28].
All in all, these results strengthen the idea that the emotional state of patients in front of a hysteroscopy is an important question to bear in mind to have good results in the procedure.
The emotional state shown by the patients could be higher during the outpatient hysteroscopy than the surgical procedure (5). It suggests that one of the most important things during any noninvasive technique is the emotional state of the patients [29].
One of the limitations of the study was that pain tolerance (EVA) was always evaluated after the surgery. It would have been interesting to evaluate pain during the different times of the hysteroscopy. With this type of proceedings, we could discriminate the difference in the pain perception before, during and after the hysteroscopy procedure.
This is an important aspect to be taken into consideration for future studies in order to investigate and assess all the factors involving in pain perception or the patients’ well-being such as rate outpatient hysteroscopy success [30].
Another limitation in our study was the lack of control in the psychiatric diagnosis. We asked about any treatment for anxiety and depression, but not about other types of psychiatric disorders. For future studies, it would be interesting to carry out a longitudinal study in which other type of measures for pain and anxiety or depression might be included.
In sum, the present study highlights the relevance of routine assessment of pain and psychological status in the outpatient hysteroscopy. We found an association between pain during the procedure and the presence of depressive symptoms before that. Most important, high levels of depression and pain during the procedure were observed in patients with a negative outcome (versus positive).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
